
Early visual symptoms of keratoconus prompt a patient to complain of a reduction in visual quality, which is not completely corrected, even with the use of new glasses. This causes frequent optical visits and changes in prescription – a result of the increasing irregular astigmatic changes underlying the disease, that are causing higher order aberrations which glasses will not correct. Undiagnosed patients at this stage often present for laser surgery consultation, seeking to improve their vision in another manner, where topographical screening typically shows posterior or inferior steepening and irregular astigmatism. Optometric diagnosis can be made using a retinoscope, where the typical ‘reflex’ becomes split, swirling, or distorted, and very difficult to objectively gauge a prescription. Moderate keratoconus may be identified using a slit lamp bio-microscope, where Vogt’s striae and prominent corneal nerves can be observed in the central cornea. In more severe cases, corneal thinning and steepening are observed, and an area of iron deposition may be seen around the base of the cone. Advanced cases display Munson’s sign – with the lower eyelid protruding as the patient looks downward, and in some cases the biomechanical endothelial stress causes an influx of fluid into the corneal stroma, causing swelling, pain and loss of transparently and visual quality.

Munson’s sign in an advanced case of keratoconus
In the early stages of keratoconus, vision is corrected using glasses or contact lenses. In some cases, the condition naturally stabilises over time but in others, the cornea continues to get progressively thinner and weaker. In some advanced cases, treatment may take the form of a full-thickness corneal graft, known as penetrating keratoplasty, where the central 7-8 mm of the cornea is removed and replaced with a healthy donor cornea. Other surgical options include partial thickness corneal grafts (lamellar keratoplasty), in which only the front-most layers of the keratoconic cornea are removed and replaced with healthy donor tissue, or the use of intra-stromal rings. In the latter procedure, ring segments, made from PMMA, are inserted into the cornea through small incisions. By careful positioning of the ring segments, the steepness of the cornea can be reduced. The technique, although somewhat unpredictable, is safe and has the advantage that it is reversible – the segments can be removed or repositioned if necessary. Corneal cross-linking is a novel therapy that aims to halt keratoconus progression by mimicking the natural stiffening of the cornea that occurs with age. The treatment uses riboflavin and UVA to create additional molecular cross-links within the tissue to stiffen the cornea and prevent further shape change.
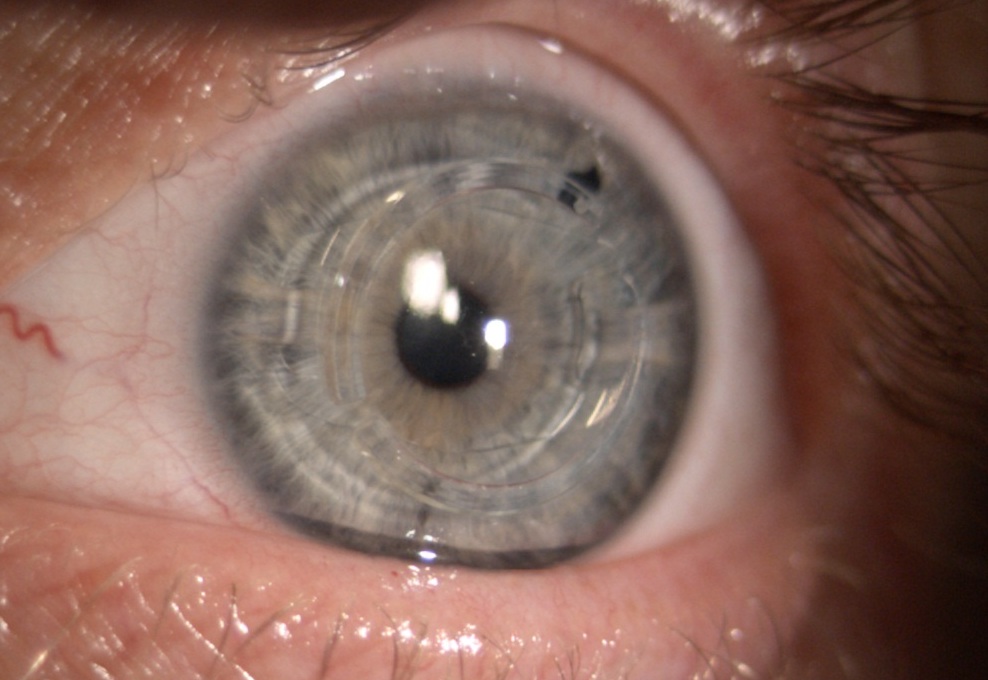
Carefully positioned intra-stromal ring segments